
Rachel Adam and Kirsty Sutter, advance spinal orthotists, Scottish National Spine Service
If you have been diagnosed with scoliosis, one of the treatment options is spinal bracing. Your spinal consultant will determine if this is an appropriate treatment for you and if so they will send a referral to orthotics. Availability and treatment may differ depending on the spinal unit you attend. An orthosis is an externally applied device used to modify the structural or functional characteristics of the neuro-muscular and skeletal systems. A spinal brace is a type of orthosis which is used to treat scoliosis. In Edinburgh, there are two types of brace that we use depending on your type of scoliosis. These are the corrective spinal brace and the postural spinal brace. The corrective brace we use is a custom made Boston Brace (Figure 1). This brace is used commonly for idiopathic scoliosis. It is worn for 20 hours per day. Commonly, the expectation is that the brace can correct the curve; however the aim is to stop or slow down scoliosis progression during a period of rapid spinal growth. In bigger curves bracing is used to delay surgery, which allows for as much natural growth and chest development as possible before scoliosis correction. This brace can be applied in children as young as 6-months-old until growth is complete. The postural brace used is a custom made two piece brace which allows for easy application (Figure 2). It is generally used for neuromuscular scoliosis and is worn during day time only. It does not correct the curve but uses the flexibility of the curve to improve the child’s sitting position. This process has many health benefits, including better respiration and digestion. Because the brace holds the child in a more upright position it also benefits eye contact, arm function, and general communication. This type of brace is worn through the day only. It can accommodate feeding tubes and can be removed for physical therapy when required. It works well alongside a supportive wheelchair. It can also be used from the point at which a good seating system is established and into adulthood.
 Figure 1. Boston Brace
Figure 1. Boston Brace
 Figure 2. Postural Brace
Figure 2. Postural Brace
Casting
Each spinal brace is custom made, and a plaster impression is taken of the child’s spine using a casting frame called the Risser Frame. The plaster cast is the same for each type of brace. Taking a cast ensures the brace will be unique to the child’s shape and as comfortable as possible. The frame also ensures the best possible position of the spine because gravity is eliminated. We apply longitudinal traction using a strap under the child’s chin, which works together with a strap around the waist to keep the child secure on the frame and in a good position. There are at least two orthotists present for this procedure and it takes approximately 30 minutes. Whilst most casts are done with patient awake as an outpatient, on occasions we need to cast a child under a general anaesthetic if their level of cooperation is poor.
Blueprinting
Once the cast has been taken it is sealed and filled with liquid plaster. This gives us a 3D model of the child’s spine to work on. The cast is adjusted to add areas of relief over bony areas, which makes the brace as comfortable as possible. The trim lines for the postural brace are generic. However, the trim lines for the Boston Brace are determined by a blueprint of the child’s most recent X-ray, which ensures that the brace targets the individual child’s curve(s) in the most effective way. A named orthotist will make the blueprint and the adjustments to the cast. The brace will be fitted approximately 4 weeks after the cast has been taken.
 The Risser Frame
The Risser Frame
Manufacture
The spinal brace will be manufactured in our in house workshop by our team of technicians. It consists of a lining material for comfort and a plastic outer shell for strength. These materials are heat moulded under vacuum to ensure an intimate fit to the cast. At this point the child’s choice of pattern for their brace is added, if the child has chosen one. The brace is then removed from the cast and trimmed to match the specified trim lines. The straps and corrective pads are added before the fitting appointment.
Fitting
The fitting appointment will last up to 2 hours and this is really important to ensure the brace fits the child comfortably. Any adjustments required will be done on the day and the family will leave this appointment with the finalised brace. The child will be given a tight fitting vest to wear underneath the brace and the rest of the clothes are worn on top of the brace. The braces are a very close fit and are not particularly visible under clothing. The orthotist will show the family how to put the brace on and take it off correctly. They will discuss how to build up optimum wear time. For the corrective brace we aim for 20 hours of daily wear, and day time wear only for the postural brace. The orthotist will discuss this with the child and their parents. The family will be given a leaflet at fitting that explains everything discussed at the appointment and there is also information available on the service’s website.
Follow-up
We have a well established routine to check the fit of our patients’ braces. The child will be seen by the orthotist and the spinal consultant about 6-8 weeks after the brace has been fitted. It is important within this time that the child establishes a good routine with the brace and reports any issues to the orthotist to allow these to be resolved. At the follow-up appointment the child will have the brace checked by the orthotist and any adjustments required will be done at this time. The child will then have an X-ray wearing the brace. It is important that the brace fits well and is fastened securely for the X-ray to provide maximum support to the spine. The spinal consultant will measure the curve(s) on the X-ray and discuss pad placement with the orthotist. There is a wire inside the corrective pads within the brace which shows up on the X-ray. If these need to be moved to optimise the support from the brace to the spine the orthotist will do this on the day. The brace must be as accurate as possible to achieve the best correction result. Corrective pads are only added to corrective braces. The child will then be reviewed 6 monthly by the consultant and orthotist and as required in between these appointments for brace-specific needs.
Below is an example of how effective corrective bracing can be. This is an X-ray of a 12-year-old patient with an adolescent idiopathic scoliosis. The patient was Risser grade 0 at the start of brace treatment which indicated a substantial amount of remaining growth (the growth plate across the upper end of the pelvis had not yet appeared). The left thoracolumbar curve measured 36 degrees before brace treatment and reduced to 6 degrees in the Boston brace. A wire can be seen in the X-ray in the brace and this is the outline of the corrective pad. This allows us to assess if the pad is in the correct position and alter it where necessary. This patient is very committed to brace wear and continues to wear it 20 hours per day without any complaints. Brace treatment for this patient will continue until the end of spinal growth and the aim is that when the brace is removed the curve will remain at least at a similar size to what it was before brace treatment, which will allow the patient to avoid scoliosis surgery.
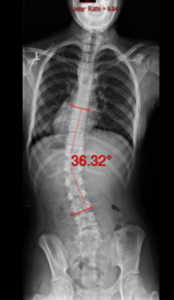 Pre brace X-ray
Pre brace X-ray
 Blue print of X-ray for brace
Blue print of X-ray for brace
 1st X-ray in brace
1st X-ray in brace
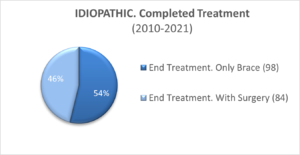
Bracing data
In Edinburgh we are part of the Scottish National Spine Service. Any child living in Scotland with a diagnosed spinal condition can be referred for treatment. We are a team of five spinal orthotists working closely with three spinal consultants and two spinal liaison nurses. The bracing results we see are reflective of a well established team approach. This financial year it is projected that we will have supplied 340 braces to patients throughout Scotland. These are a mixture of corrective braces and postural braces. We recently looked at our data over an 11-year period that included 480 patients treated with a Boston Brace (corrective brace). Of the patients who have an idiopathic scoliosis our figures show that 54% of these patients did not require surgery at the end of brace treatment. For the 46% of patients who did require surgery brace treatment delayed spinal surgery for several years, preserving the growth of their spine and chest development. All patients who had completed treatment filled out a questionnaire about brace treatment. They reported normal function, good self image, and reduced pain, as well as high satisfaction in the group who required bracing only and those who required bracing followed by scoliosis surgery.
Patient comments:
“The orthotic service for my child’s brace has been exceptional. Despite having some doubts about my son wearing a brace for his scoliosis, he has managed his daily activities well beyond my expectations. The constant communication and feedback from the orthotics and spinal team has been amazing and has established my trust. The team on board with my son is phenomenal. I would like to thank our orthotist and consultant surgeon for their work in helping my son cope with his brace”
“My child has been in her brace since she was 2. It was a big adjustment but gradually it just became part of everyday living. The orthotic team spend time making sure she is comfortable in the brace at every visit, especially when getting a new brace. She has coped well with the brace and we gave it a nick name ‘Bear’ because she was so young and thought it would help. Now she is 13 and it is still called Bear sometimes. The spinal service has been great. We are able to contact them if adjustments are needed and they are very accommodating with appointments around my work commitments. My child is still in her brace 20 hours per day and this has helped keep her spine as straight as it can be. The spinal team is great”.
“Our daughter has been braced for about a year now and has adapted well to wearing her brace full time. Although it is going to be a long journey, our experience of bracing so far has been positive. She is a very active 3 year old who loves to swim, dance, and go to gymnastics. The brace can be removed for a maximum of 4 hours each day, which allows her to fully participate in all the activities she enjoys. We are extremely grateful that she has this time out of the brace since not only is it important for her to physically exercise, but also for her overall wellbeing. The standard of service we have received from our daughter’s consultant and The orthotics team in Edinburgh has been outstanding. Nothing is ever too much bother and they always take time to explain any questions we have. With their support and expertise, we feel confident that our daughter is in safe hands”.
We would like to thank our patients for their feedback and for allowing us to use their photographs and X-rays for this article
– Rachel Adam and Kirsty Sutters.